


Causes of cervical cancer, 'HPV', the vaccine
and vaccine induced illness.

How does cervical cancer develop?
A quick recap to begin. The cervix is the gateway to the womb from the vagina.
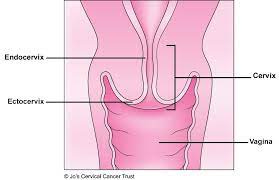
The vagina has squamous epithelium, a skin like protective layer, a few cells thick. The cervix has mucus producing glandular cells and is thinner. Hormonal changes cause the cervix to evert during puberty.

The transformation zone of the cervix is where the epithelium changes from the squamous protective layer, on the left, to the more vulnerable and thinner layer of glandular cells, on the right.
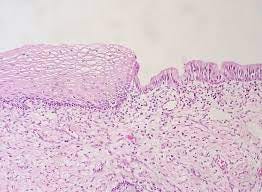
Lesions and cancer are most likely to happen in the transformation zone, which is why this area is sampled on a smear, as these cells can change into either cell form depending on hormonal and other factors.
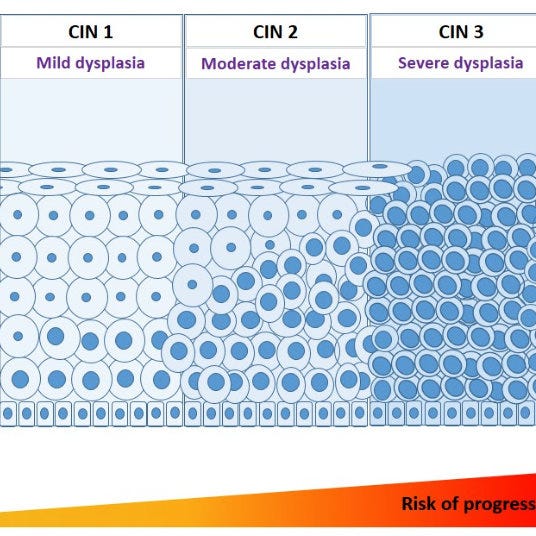
Smear tests pick up dysplasia (abnormal changes in cells) which indicate pre-cancers (they may or may not become cancer). These changes are known as CIN which refers to Cervical Intraepithelial (within the epithelium, not invasive, unable to metastasise) Neoplasia (new growth). CIN has 3 categorises depending on the extent of the changes seen in cells, which corresponds to thirds of the epithelium
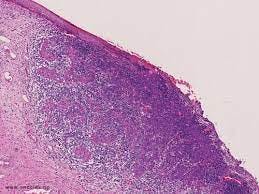
Repeated CIN on cytology (cells) is followed up with biopsy and is confirmed with histology (tissues). Finally a Laser Loop Excision of the Transformation Zone is performed.
Why is screening and treatment for cervical cancer potentially effective?
a) The cervix is accessible for sampling and surgery without needles, cutting, crushing or harmful X rays.
b) The cancer is localised to one particular area of the cervix and once removed, if caught before it has spread through the basement member, the cancer is effectively cured.
Is screening effective?
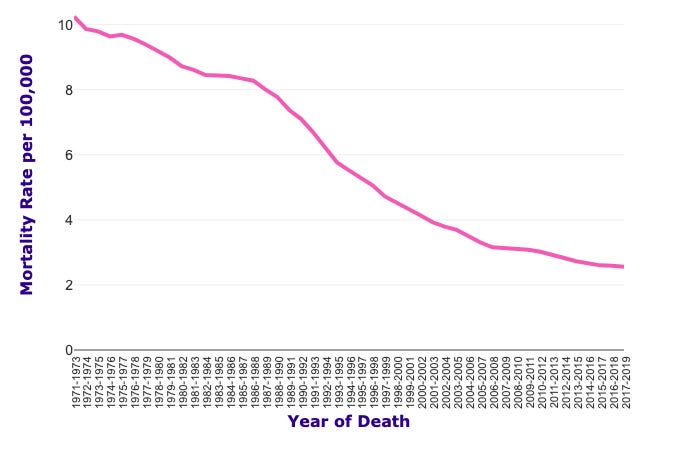
Screening was first introduced in the UK in 1964. Surgical intervention from observing CINs through screening in England in this paper show a 75% reduction in cervical cancer deaths. However, the paper is not randomised and compares those who self-select for screening with those who don’t. In another study of UK wide cervical cancer in women there were about 10 in 100,000 deaths at the beginning of the 70s and about 4 in 100,000 in 2017-19, an absolute reduction of 0.006%, or 1950 lives saved in the UK female population as a whole. The deaths are age adjusted and although other factors maybe involved, such as hysterectomies (though these have decreased with the rise of ablative surgery), a major influence must be cervical screening.
Cervical Cancer (C53), European Age-Standardised Mortality Rates per 100,000 Female Population, UK, 1971-2019

What are the risk factors for cervical cancer?
The three main risk factors for developing cervical cancer are a) smoking, b) young age of first intercourse and c) low socio-economic class.
a) Smoking needs no further explanation. It’s not good for you, don’t do it.
b) The age of first intercourse is significant as the cervix is only fully developed through the hormonal changes of puberty. Semen is very oxidising and may cause changes in the undeveloped cells of the cervix as a protective response.
c) Socio-economic class would indicate that nutritional factors, such as access to fresh fruit and vegetables, and other life-style factors such as housing, air quality and exercise are important in the development of cancer.
There is also indication that other are beneficial practices are a) avoiding intercourse during menstruation, when hormonal and cellular changes are occurring and b) avoiding bacteria and toxins found in smegma by regular washing of the penis or by circumcision.
What is cancer?
Some postulate that cancer itself is a healing and protective mechanism that occurs in response to toxins, stresses, nutritional deficiencies or other traumas. The morbidity and deaths due to this ‘cancer’ may be caused by the continuing assault of the trauma which the body is unable to cope with or by the treatment, such as chemotherapy.
What is ‘HPV’?
When was ‘HPV’ discovered and how was it ascertained that is caused cervical cancer? In the 1990’s when PCR tests started being used some novel DNA sequences were found that were strongly associated with cervical cancer. These sequences were called human papillomavirus; though they have never been shown to be part of a single entity, nor that the entity is transmissible nor infectious, nor that the entity causes cancer.
The sequences are only associated with cancer, not causative. They are also found in 80% of women at some point in their lives and, as we have seen, only 0.01% of women were dying of cervical cancer at the beginning of screening. Just like with HIV and AIDS there is no paper that shows ‘HPV’ is the probable cause of cervical cancer.
Some of the ‘HIV’ sequences and proteins (p120, p42 and p25) have been found in breast, ovarian and prostate tumours but not in surrounding normal tissue; they were also detectable in the blood. Could these sequences and proteins, plus any virus-like particles (the spore-like bacteriophage and tobacco mosaic ‘virus’ are produced by bacteria and plants under stress) associated with ‘HIV’ and ‘HPV’ be produced by the body under stress as part of the survival or healing process and be used as a diagnostic indicator and impetus for a change in lifestyle?
One can’t just dismiss this phenomenon by saying that the PCR is fraudulent and can be misused. The PCR technique provides high fidelity in amplifying the sequences it’s primed for and the adjacent normal tissue to the tumours provides the best negative control one can possibly wish for. Yes, ‘HIV’ is found in inflammatory conditions, pregnancy and healthy people, yes ‘HPV’ sequences are found in 80% of healthy women. However, their sequences are found repeatedly in breast cancer and cervical cancer tumours respectively but not in the surrounding tissues. The ELISA technique could potentially be used (if one is OK with using animals) to assess the amount of these sequences not just their presence, which would be far more useful. If everyone was not obsessed with sexually transmitted diseases, viruses or disproving viruses maybe we could find out what these sequences do in fact represent.
Is the ‘HPV’ vaccine effective?
The HPV vaccine introduced in 2008 in the UK. Not surprisingly, as HPV has never been shown to cause cancer, the vaccine has never been shown to prevent cancer. In Australia the first country to introduce Gardasil in 2006 cancer incidences in young women increased between 1982 and 2017.. This could be due to a decline in screening following the roll out of the vaccine supposed to prevent cancer or it could be the toxic effect of the vaccine itself. Either way it did more harm than good.
Another study claims to show that the vaccine has a 75% efficacy at preventing the so-called precancerous lesions, CIN. It does not. The efficacy they refer to is relative, the absolute efficacy for women vaccinated at 16 or younger for CIN2 was 1.98% (that is 2% of women developed CIN2 in the unvaccinated group and 0.02% in the vaccinated) and for CIN3 was 0.0096%. CIN’s are mostly likely to occur in young women, so the apparent benefit of vaccination disappears for later ages.
The study is not a randomised nor placebo controlled, it is only observational of self-selected groups. The unvaccinated group had 17 times more parents with very little education and nearly 4 times more had only reached high school than in vaccinated group. Nearly 60% of the vaccinated group parents had university educations compared to 40% in the unvaccinated group. It is entirely plausible that socio-economic factors played a large part in the outcomes. Smokers, girls having sex at younger ages, those less well nourished and with less well educated parents (in the case of the vaccine; very fortunately for their child) are over represented in the self-selected unvaccinated cohort.
This study cannot even show the vaccine has the claimed 1.98% benefit at preventing CIN, let alone cancer. There is no evidence from a randomised, placebo controlled trial that the vaccine has any efficacy whatsoever.
Is the ‘HPV’ vaccine harmful?
There is much evidence that the HPV vaccine causes debilitating conditions such as POTS and other ‘autoimmune’ diseases; which are really effects of vaccine toxins on the homeostatic mechanisms of the body. Please see ‘The HPV vaccine on trial; seeking justice for a betrayed generation’ by Iorio, Rosenburg and Holland.

Conclusion.
Just like HIV and the real causes of AIDS; poverty, malnutrition, recreational drugs, lack of sleep and AZT; the real causes of cervical cancer; smoking, early first intercourse and lack of fresh fruit and veg are ignored at the expense of pouring $billions into the vaccine, which itself goes on producing more clients for pharma.
🐒
Interesting theory about semen being an oxidizer. That probably explains why 1) condoms are associated with reduced risk for cervical cancer, despite 2) the claim that condoms don't protect against HPV, or at least not very well, as it can sneak right around them from areas not covered. Your theory is far more elegant.
As the door opens wider, we see dark and deep the insanity is.