
The MMR and Autism
Pharma's $billion cash cow we're not allowed to mention


What is the evidence that the MMR is damaging to health or that it may cause autism?
Autistic Spectrum Disorder is an umbrella term referring to a range of social, communication and behavioural disorders. The interaction between a child and his or her parent at crucial stages of brain development causes synapses controlling social interaction and dopamine pathways to form. These synapses and acquired brain interconnections seem to be hindered in children with ASD. Autistic people are not defined by their diagnosis but the term is used for the purpose of study.
‘In 1943, a famous paper was published in which Leo Kanner, a child psychiatrist at Johns Hopkins, described a series of children with “fascinating peculiarities.” He thought that “these characteristics form a unique ‘syndrome,’ not heretofore reported, which seems to be rare enough, yet is probably more frequent than is indicated by the paucity of observed cases.” He called the syndrome autism.
What causes autism? “It is now broadly considered to be a multi-factorial disorder resulting from genetic and non-genetic risk factors and their interaction.” Autism spectrum disorder (ASD) can run in families, but genetic factors may account for only 10 to 20 percent of cases. This is based partly on the fact that you can have identical twins with identical DNA—the exact same genes—and one twin may have autism, but not the other. “While genetic susceptibility may be a key contributor to ASDs, it may conceptually just ‘load the gun’ so to speak, with prenatal, perinatal, and/or postnatal environmental exposures”—that is, environmental exposures during, around, or after pregnancy—“being the events that ‘pull the trigger’ and may give rise” to the disease.’
Has ASD been increasing?
Autism didn’t even have a diagnosis until 1943 so there could have been loads of it before hand and it just wasn’t noticed. Or their could have been very little of it and it’s recently increased. However, ‘while we may never really know what the prevalence of autism was a half century ago, we do have decent data over the last few decades that do point to a considerable increase in the true prevalence.
Maybe there wasn’t actually a 22-fold increase in autism in the 1980s and 1990s. Maybe there was actually only an eightfold increase. We may quibble over whether the increase was 800 percent or closer to 2000 percent, but it seems that autism rates truly are increasing, so the question legitimately turns to why?’
John’s Hopkins branch of pharma marketing says ‘we are seeing is a gradual rise over the past 20 years due to broadened diagnostic definitions, better screening, and increased awareness.
There are still a large number of people in our community with autism, and our focus should be on getting them the services they need to lead healthy lives and reach their full potential.’
And even if ASD hasn’t been increasing; don’t we want to know what causes it when it does happen? Finding the cause may not be the top priority for parents of autistic children, the horse has already bolted; ‘Other consultations have suggested that finding causes is not a priority for some autistic people. In 2016, Autistica and a group of other UK autism charities consulted more than 1,000 autistic people, their families and professionals and asked them to devise a top-ten list of questions they wanted research to answer. It included finding ways to improve and support mental health, communication, education and other needs. None of the listed priorities was about finding causes of autism.’
There is also little appetite among researchers on autism to prevent it and thus do themselves out of a job or career. Nor is there funding coming from big pharma whose products may be implicated in causing it, but crucially their profits from autism drugs will be harmed by preventing it.
However, if I was thinking about getting pregnant- I’d damn well want to know the risk factors.
What causes ASD?
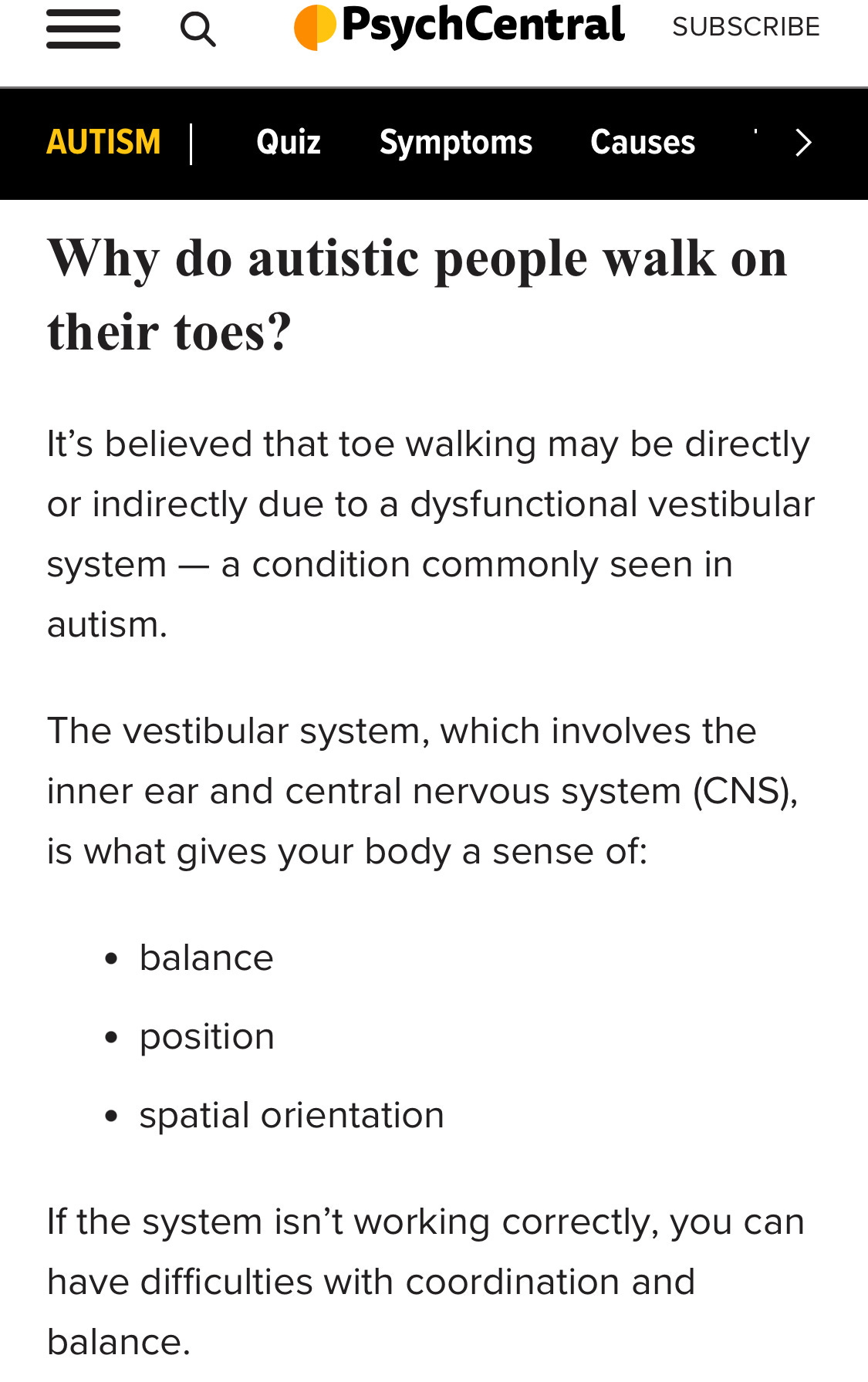
Autism is associated with vestibular dysfunction and with frequent ear ‘infections’.
Ear problems, perinatal ‘precautionary’ use of antibiotics, birth method, being male and black plus having vaccinations all seem to be risk factors.
The gastroenterologist Andrew Wakefield noted that autistic children made up a significantly larger percentage of his referrals.(1) Indeed GI co-morbidities have been reported in 9-91% of ASD patients and the prevalence of symptoms four times greater than in children without ASD(2). Wakefield collected the data from a study involving other doctors and their patients (the Lancet 12). When asked for their histories some of the parents of the patients noted that ASD symptoms had started not long after the MMR vaccine (and that a possible link had been denied by their GP’s and their concerns poo pooed).
Wakefield writes: ‘On March 6, 2004, some of our ex-colleagues issued a “retraction of an interpretation”, not a retraction of the factual content of the paper, as widely inferred. Since no interpretation of the possible MMR/autism link was offered in the original 1998 Lancet report, other than to state that the data did not constitute evidence of an association and suggest that further research was required, it is difficult to know quite what has been retracted, particularly in light of Richard Horton's current plea for further research funding for autism, a plea that we welcome wholeheartedly.’
Let us be clear that parents reported gastrointestinal symptoms in their children that many medical professionals denied and refused to investigate. Some parents were referred to social services and false claims of Munchausen's syndrome by proxy were levied. The parents were right; their children have an inflammatory intestinal disease. The medical profession was wrong, in some cases shamefully so. In light of this lesson it is imperative that rather than relying on endless reviews of epidemiological data which fail to even address the original hypothesis,4 parental claims should be taken seriously and their children should be investigated on an individual basis.’
Wakefield goes on ‘The full story has yet to unfold. In a timely BMJ newspeice, Begg who is described as a leading virologist, calls for MMR research to be terminated on the basis of Taylor and co-workers' report and a non-peer-reviewed so-called analysis in Current Problems of Pharmacovigilance. Clearly there are some things that may end-up being terminated as a consequence of these events: research into the possible link between MMR, autism, and bowel disease is not one of them.
Taylor et al tested the hypothesis that there should be no temporal clustering of first parenteral concerns with measles, mumps, and rubella (MMR) vaccination. They identified a statistically significant excess risk by 6 months after MMR, which they dismiss, post hoc, as indicating parental recall bias. Had this been the case it should have been seen in both of their vaccine groups—those receiving MMR and those receiving any measles-containing vaccine. The excess risk was seen only in the MMR group; this is a fundamental flaw.
However, it pales into insignificance compared with their failure to declare the fact of an MMR catch-up campaign that was initiated in 1988 with the introduction of this vaccine. This campaign was targeted at children, whatever their age, who presumably had not received either monovalent mumps or rubella vaccine whatever their exposure status. As such it was a novel and, in terms of safety, untested policy. On the basis of Taylor and colleagues' inclusion criteria, and taking account of the catch-up campaign, then those first birth cohorts who actually received MMR (circa 1986) were precisely those in whom a doubling of the numbers of cases of autism were seen. Thereafter these numbers continue to increase strikingly. Omission of this essential fact—the catch-up campaign—requires explanation lest it be misconstrued.’
A journalist, Brian Deer, writing for the BMJ no less, called Wakefield a fraud who had deliberately falsified the Lancet 12 data to appear in a lawsuit. Wakefield replied ‘Conflict of interest is created when involvement in one project potentially could, or actively does, interfere with the objective and dispassionate assessment of the processes or outcomes of another project. We cannot accept that the knowledge that affected children were later to pursue litigation, following their clinical referral and investigation, influenced the content or tone of the 1998 paper which was a description of a possible new syndrome in the classical mode. We emphasise that this was not a scientific paper but a clinical report. The laboratory support funded by Legal Aid for a separate viral detection study had no bearing on the original paper. No Legal Aid money was used in the preparation of the 1998 paper, and the viral study could not then and indeed, does not now, influence the “objective and dispassionate assessment” of the veracity of the original paper, which we reiterate simply reported a novel clinical syndrome. There was no conflict of interest.’ He also sued the BMJ for defamation.
Deer allegedly tracked down the parents of the 12 anonymised children. One of the parents who had been told his son wasn’t part of the study was convinced by Deer that he was. He made big of the fact that Wakefield’s colleague had recorded, in consultation with his parents, who believed vaccines were to blame, symptoms as appearing at 15 months.The whole reason that the 5 year old child had been flown from California to the Royal Free in London was to be part of a study on vaccination. The parents noted the symptoms happened after the 13 month check up, which was normal, and the report in the Royal Free discharge notes was: “In the period 13-18 months he developed slow speech patterns and repetitive hand movements. Over this period his parents remarked on his slow gradual deterioration.” There are other trivial discrepancies, if the child is indeed the anonymised child 11, that do not affect the overall findings of the study.
Deer also harassed the mother of child 2 (she called him the gutter press and complained to Deer’s editors) over her child’s confidential medical information and her account of the onset of their symptoms. Her account allegedly does not match with any in the paper. Deer hounded her to say whether it was 2 months or 6 months after vaccination that her child developed symptoms. This was recorded by Wakefield’s colleague as 2 weeks (even if symptoms did occur 6 months after vaccination, it doesn’t mean vaccination was not responsible). Deer claimed that Wakefield had phoned the mother of child 2 prior to the consultation and ‘suggestively questioned’ her. The exact same allegations of fraud were levelled against senior Doctor (with better paid lawyers) Walker Smith, who was cleared of all charges.
Vera Shervav says 'I have undertaken this review of the case against Dr. Andrew Wakefield because the issues involved are far more consequential than the vilification of one doctor. The issues, as I see them, involve (a) collusion of public health officials to deceive the public by concealing scientific evidence that confirms empirical evidence of serious harm linked to vaccines – in particular polyvalent vaccines; (b) the “willful blindness” by the medical community as it uncritically fell in line with a government dictated vaccination policy driven by corporate business interests.
Public health officials and the medical profession have abrogated their professional, public, and human responsibility, by failing to honestly examine the iatrogenic harm caused by expansive, indiscriminate, and increasingly aggressive vaccination policies. On a human level, the documented evidence shows a callous disregard for the plight of thousands of children who suffer irreversible harm, as if they were unavoidable “collateral damage”.
All of the documented evidence and testimonies submitted to the General Medical Council, upon which GMC issued its guilty verdicts against Dr. Wakefield and his two co-defendants in 2010, were subsequently forensically assessed by the UK High Court in March 2012, in the appeal of Professor John Walker-Smith, the senior clinician and senior author of the Lancet case series. The High Court determined that the verdicts of professional misconduct and ethics violations were unsupported by the evidence.
Indeed, the adjudicated evidence refutes the case against Dr. Wakefield; the documents and testimonies demonstrate that there is no evidence whatsoever, to support the charges of professional misconduct, much less the accusation of fraud.
The accusation of fraud was hurled by the Editor-in-Chief of the BMJ, a medical journal whose corporate ownership is intertwined with the vaccine manufacturing Behemoths, Merck – with whom BMJ signed a partnership agreement in 2008 – and GlaxoSmithKline which provides additional financial support to BMJ. Among their numerous vaccine products, Merck and GSK manufacture the MMR vaccine.’
The BMJ editors think that we should all stop wasting time. ‘But perhaps as important as the scare’s effect on infectious disease is the energy, emotion, and money that have been diverted away from efforts to understand the real causes of autism and how to help children and families who live with it.’ The three BMJ editors say ‘One clue (as to the public’s distrust caused by the Lancet 12) comes from an outbreak in a school in Essen, Germany, attended by children whose parents were opposed to vaccinations. Of the 71 children infected with mumps, 68 had not been immunised.’ Hurrah for them! ‘Mumps’ as a child is a detox phase that protects them from later illnesses. Exasperation and emotional blackmail being used by pharma to protect their useless and harmful products.
‘Deer shows how Wakefield altered numerous facts about the patients’ medical histories’. Wakefield’s hypothesis (that’s all it was) of a new bowel/measles virus/MMR/autism syndrome doesn’t seem to hold water. Which is fine. That’s what science is for. However, he didn’t claim that the paper proved his new syndrome nor even showed an association between the MMR and autism. Yet, the witchhunt of Wakefield is used by the pharma funded BMJ, to continue claiming that Wakefield is a fraud.
‘Who perpetrated this fraud? There is no doubt that it was Wakefield. Is it possible that he was wrong, but not dishonest: that he was so incompetent that he was unable to fairly describe the project, or to report even one of the 12 children’s cases accurately? No. A great deal of thought and effort must have gone into drafting the paper to achieve the results he wanted: the discrepancies all led in one direction; misreporting was gross.’
This is outrageous. Wakefield merely collated the reports from his colleagues. There is no evidence of ‘falsification’ as claimed by the journalist Deer. The hoohaa that the study didn’t have ethical approval (it was just a report, so it did) and that it was part of a lawsuit (it wasn’t) is being used as proof that the MMR has been exonerated. It’s so rich that pharma and regulation call fraud (even though the High Court found no evidence) when they themselves pay $billions in fines for misrepresentation and fraud.
It has apparently been shown in RCTs that the MMR vaccine and the onset of ASD symptoms are not correlated. However vaccines are not tested against saline placebos. The same ‘immune’ stimulating adjuvants (containing known neurotoxins aluminium or mercury) are used in the placebo arm as the treatment arm, so that all adverse reactions caused by them are masked during trials.
What about the Cochrane Review?
The Cochrane Review apparently exonerating the MMR and autism, only looked at 7 observational studies involving vaccination of ‘healthy’ children. The Lancet 12 would have been excluded from the study. It’s a mockery of allegedly providing evidence of safety. It is also known that extra concentrated MMR doses (from the bottom of the vial, if not shaken properly between doses) or accidental double doses are sometimes given. It is also common practice to receive more than one type of vaccine during a single doctors appointment. The vaccines contain known neurotoxins such as aluminium.
It doesn’t matter how many millions were in the studies and though all of the individual studies were funded directly or indirectly by the pharma industry themselves, the point is that only children healthy at the time of vaccination were included. The strength of the evidence for the differences between the self-selected vaccinated was judged by the Cochrane Review to be moderate, low or very low.
The Cochrane panel initially found a great many problems with the very studies they later whitewashed in the updated April 2020 version. This is very interesting timing: just before the biggest vaccination campaign in history.
‘Indeed, the Cochrane reviewers confirmed that the scientific integrity of the studies was undermined by: “bias in the selection of controls”; “lack of a properly constructed causal hypothesis”; “extensive under-counting of autism cases in the MMR group”; “unequal length of follow-up”; “missing 14% to 20% of original birth cohort”; “between 11% and 20% of adverse event data was missing”; and in CDC’s 2004 study (Pediatrics,) “more than a third of cases were excluded”. (Cochrane MMR Reviews, 2005; 2012.)
Internal CDC correspondence, confirms that relevant findings documenting an increased risk of harm were deliberately omitted from the published and widely cited reports and even when scientists requested the full dataset of CDC’s own epidemiological study for independent analysis, CDC claimed that the data was “missing.”
Psychiatrist Poul Thorsen, MD, who was the principal Danish investigator of the Danish series of studies commissioned by CDC, failed to obtain ethics committee approval for key CDC-sponsored epidemiological studies – as is required under US and Danish law. Newly obtained internal CDC documents provide evidence of collusion and malfeasance by public health officials who attempted to cover-up those violations of legally mandated ethics committee review and approval.’
Cochrane is not an independent body. It’s funded by the US, British and Danish governments on behalf of big pharma. Governments are legally obliged to buy products from pharma under WHO law and also provide them with indemnity. Many politicians are share-holders of or are financially supported by pharma. Government regulators have a career revolving door with pharma.
The results of the studies on ASD in the Cochrane report actually show a protective affect of the MMR in reducing autism from 0.451% to 0.419% in children overall (in 1999), and from 1.2% to 0.9% in the high risk group! (the actual rate of autism in the US is now 1 in 36 ie 2.7%). This screams bias. ‘Regarding the meta-review by Taylor-three of the studies show apparent protective effect of MMR vaccines against autism (Madsen 8%, Smeeth 14% or 22% and Mrozek-Budzyn 83%!!!) which suggests bias.’ The authors admitted to indication bias in the high risk groups, ie having older siblings with ASD makes one less likely to be vaccinated but more likely to have ASD (the fact that other things such as diet, pesticides and pollution can cause autism as well, doesn’t alter the fact that the MMR or vaccines do).This highly skews the results.
The unvaccinated groups were generally much smaller so the inclusion of these extra ASD children makes a bigger difference, making the larger vaccinated group look better. In the main Danish study there were 53 ‘unvaccinated’ vs 263 vaccinated with autistic disorders and 77 ‘unvaccinated’ vs 345 vaccinated with spectrum disorders. There would also have to be an accurate assessment of what percentage of the population was ‘unvaccinated’ and what that means. The authors also make the results sound grander as those with ASD were drawn from the general population of 1 million. The authors have demonstrably not shown that the MMR is safe to use in the higher risk groups.
There’s also evidence that black male toddlers are 3 times at risk of autism from MMR vaccination at 36 months of age, in recent news a whistleblower says:
‘“I regret that my coauthors and I omitted statistically significant information in our 2004 article published in the journal Pediatrics. The omitted data suggested that African American males who received the MMR vaccine before age 36 months were at increased risk for autism. Decisions were made regarding which findings to report after the data were collected, and I believe that the final study protocol was not followed.”’
Of the Madsen paper Cochrane 2005 warned:
“The follow up of diagnostic records ends one year (31 Dec 1999) after the last day of admission to the cohort. Because of the length of time from birth to diagnosis, it becomes increasingly unlikely that those born later in the cohort could have a diagnosis”
It remains troubling that as with a number of studies from this Danish group the co-ordinator on behalf of US Centers for Diseases Control, Poul Thorsen, is wanted for financial fraud from the CDC, though not extradited to the US now after nearly 8 years.
Of the De Stefano paper Cochrane commented:
“The conclusion, however, implied bias in the enrollment of cases which may not be representative of the rest of the autistic population of the city of Atlanta, USA where the study was set.”
And indeed in 2014 the paper was repudiated by one of the leading authors, William Thompson. The study by Smeeth is compromised by its patchy data source, the General Practice Research Database where the autism rate represented is perhaps only one tenth of cases diagnosed. Cochrane commented:
“In the GPRD – based studies (Black 2003; Smeeth 2004) the precise nature of controlled unexposed to MMR and their generalisability was impossible to determine…”
It remains problematic whether the unvaccinated in this study were genuinely unvaccinated.
Of the Uchiyama study Cochrane commented:
“The cohort study of Uchiyama 2007 was potentially affected by a different type of bias, considering that the participants were from a private clinic and that definitions of applied Autistic Spectrum Disorders (ASD) diagnosis and of methods used for ASD regression ascertainment were not clearly reported.”
And the Uno study will suffer from similar issues since the cases came from the same clinic. Moreover, in both instances the studies were far too small (904 persons and 413) to necessarily provide any clear result even if they had been better controlled.
Nor can the Taylor meta-analysis cover up the entire absence of pre-marketing studies. In 1988-9 when the British government was persuaded to introduce Pluserix, MMR2 and Imravax there were no safety studies at all, and successive governments have been forced into the defence of a policy which they had embarked on without safety evidence…’
Many studies also claim that there’s no link between GI symptoms and autism, clearly false. Perhaps this confusion arises if looking just at Crohn’s and UC which show no children in either the vaccinated nor unvaccinated cohorts in the general population.
There needs to be a study looking at the MMR vaccination risk and ASD of the ‘high risk’, ‘unhealthy, ie those with frequent ear ‘infections’, siblings with ASD or on frequent antibiotics. As a bonus this cohort needs to be compared with populations that haven’t had the MMR, or any of the plethora of vaccinations even before the MMR at 12-18 months, as a general risk factor. Comparing the ‘unvaccinated’ with the ‘vaccinated’ is similar to comparing 20 cigarettes a day with 21, or 2 rashers of bacon a day with 2 and 1/2- and seeing no difference.
The pharma industry has used the same playbook as the animal ag industry; comparing highly vaxxed kids (or high saturated fat diets) with highly vaxxed kids (or high saturated fat diets)- and seeing no difference.
What about studies that do compare unvaccinated children?
‘DTP or tetanus vaccination in US children is associated with life- time history of asthma or other allergies and allergy-related symp- toms. . . . Assuming that the estimated vaccination effect is unbiased, 50% of diagnosed asthma cases (2.93 million) in US children and adolescents would be prevented if the DTP or tetanus vaccination was not administered.’
‘This study found statistically significant evidence to suggest that boys in United States who were vaccinated with the triple series Hepatitis B vaccine . . . were more susceptible to developmental disability than were unvaccinated boys. . . . The odds of receiving EIS [special education] were approximately nine times as great for vaccinated boys (n = 46) as for unvaccinated boys (n = 7), after adjustment for confounders.’
‘The vaccinated were less likely than the unvaccinated to have been diagnosed with chickenpox and pertussis, but more likely to have been diagnosed with pneumonia, otitis media, allergies and NDD [neurodevelopmental disorders]. After adjustment, vaccination, male gender, and preterm birth remained significantly associated with NDD.’ Specifically, vaccinated children were found to have a fourfold higher likelihood of having autism.
‘Preterm birth coupled with vaccination, however, was associated with a synergistic increase in the odds of NDD, suggesting the possibility that vaccination could precipitate adverse neurodevelop- mental outcomes in preterm infants. These results provide clues to the epidemiology and causation of NDD but question the safety of current vaccination programs for preterm infants.’ The results were disturbing, as the researchers found children born prematurely and vaccinated were fourteen times more likely to develop a neurodevelopmental disorder!
‘Within this study, the number of vaccines received and vaccination status early in life are related to different acute and chronic conditions. The strongest relationships observed for vaccination status were for asthma, developmental delays and ear infections.’ From “Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders,”
‘“…this large-scale birth cohort study demonstrated that the prevalence of asthma, wheeze and eczema in children at 12 months of age was associated with the administration of a larger number of types of inactivated vaccines at the initial immunisation before 6 months of age.”
‘Studies that might hurt the financial performance of pharmaceutical companies are not publicized by media outlets that derive advertising revenue from the pharmaceutical companies.’
A brilliant run down here of the July 2025 Danish paper apparently exonerating aluminium in vaccines. When you exclude the factor that you’re looking for and lump the unvaccinated in with the low dose cohort you get the absurd result of finding that aluminium improves asthma and autism.
‘Briefly, the authors chose to
examine very young children (thus those having little aluminum exposure from vaccination)
only consider outcomes early in life
exclude kids who were potentially showing signs of aluminum toxicity early
exclude kids who potentially received the most vaccinations of all
confine the primary analysis to searching for outcome differences as a function of small differences in exposure
inappropriately adjust for propensity to seek medical care and
bury what could have served as a large control group among a much larger group of vaccinated kids.’
What other factors may cause ASD?
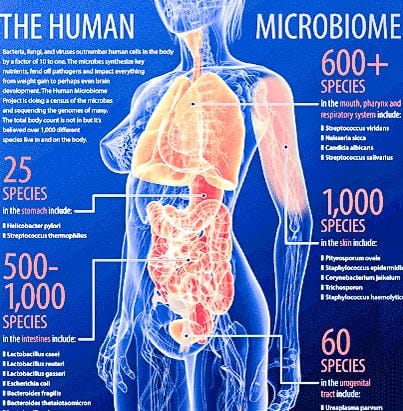
The beneficial gut bacteria, especially Prevotella sp are fibre loving. As fibre is only found in plants, a diet rich in fruit, veg and legumes is essential. People with ASD have less Prevotella. As autistic people tend to be ‘picky eaters’- whether cause or effect is unknown- this can be a challenge. My experience with people with learning disabilities showed me that they universally had poor diets, consisting mainly of junk food, crisps, white bread and processed meat. Protocols have been devised to help with picky eating. For example committing to trying one new food a day. Fecal transplants from fibre eating healthy individuals into ASD patients significantly improves behavioural symptoms.
Supplementing with compounds found in broccoli sprouts also improves disruptive behaviour, social interaction and verbal communication, possibly by decreasing oxidative stress and neuroinflammation, increasing glutathione and mitochondrial function and thus allowing the crucial synapses in the brain to form connections. The benefits were reversed with the supplementation was discontinued (3). Supplementation with broccoli sprout extract would seem to be a completely safe treatment which would not react with any drugs already being taken. In contrast Bacteroides and bilophilic bacteria associated with high meat and high fat diet appear to decrease gut barrier integrity and cause putrefaction in the colon exacerbating ASD symptoms.(2)
The way food is produced and the health of the microbiome in the soil is also crucial. Bacteria and plants can pass genes, such as antibiotic or herbicide resistance, by just being next to each other. This means that weeds around GMO crops must be sprayed with increasing numbers of different types of weed killers. Glyphosate works by disrupting the shikimate pathway (found in plants and bacteria but not in humans) which creates the essential amino acids phenylalanine, tryptophan and tyrosine.
Continual use of herbicides and fertilisers, with no green manure rotation, destroys the microbiome and depletes the soil, meaning that humans and animals are eating malnourished plants. Humans become sick and are treated with yet more pharmaceuticals. The incidence of autism has increased in line with the increasing use of glyphosate.
A healthy microbiome in humans not only protects the gut lining. It crucially protects the blood/brain barrier. The brains of babies and children are constantly developing, growing and, as they interact with other people, creating synaptic connections that control social interaction and behaviour. The brains of those children unfortunate enough to have fever or diarrhoea from vaccinations including the MMR at an early stage of development at the same time as a course of antibiotics (or who frequently have them) or who are taking certain pain killers, will be particularly vulnerable to the vaccine as the blood/brain barrier protection is compromised. There’s also evidence that casomorphins from cow’s milk affect GI integrity and lead to the behavioural symptoms associated with ASD.
How prevalent is ASD?
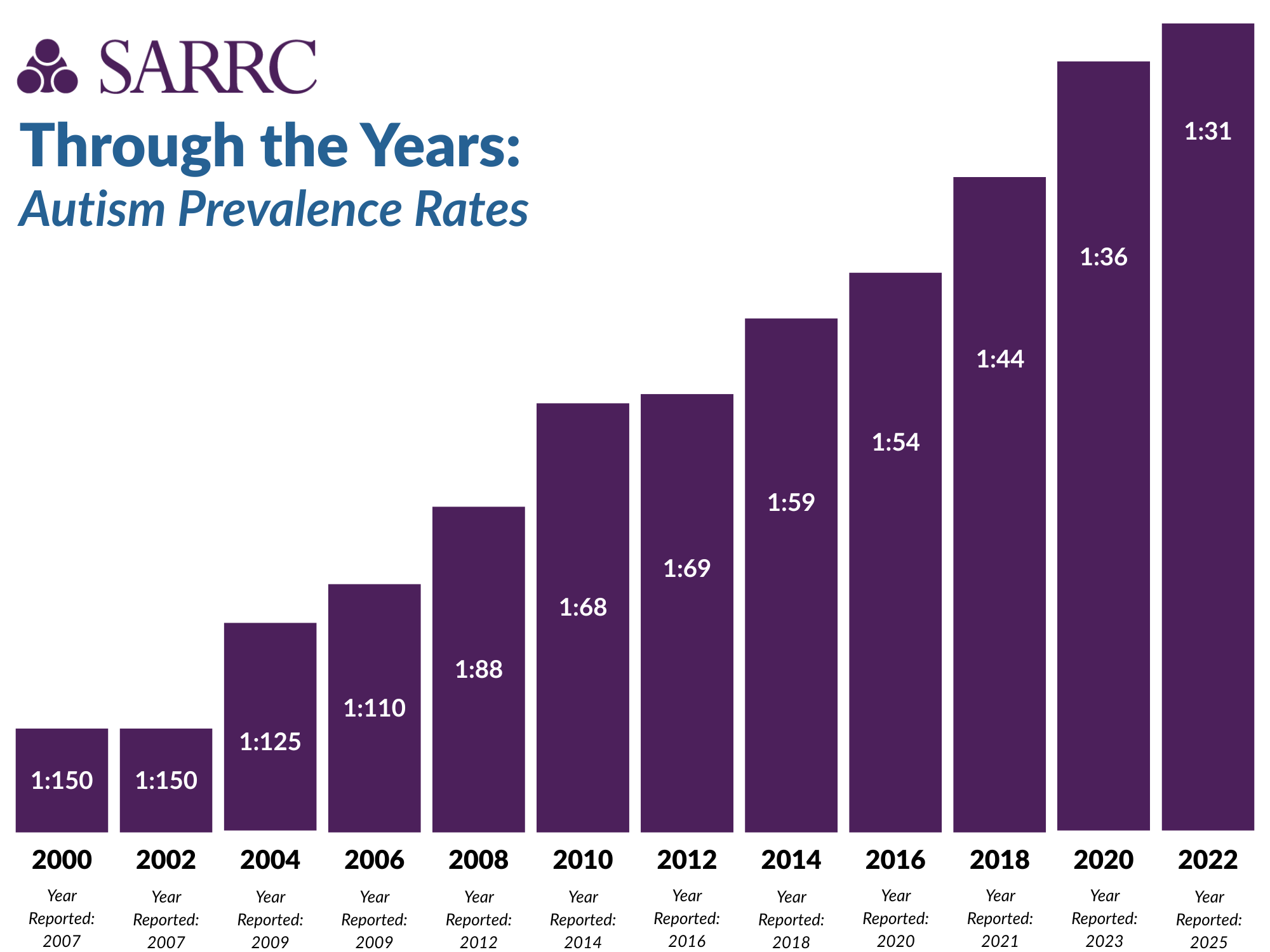
Autism is now estimated to affect 1:31 children in the US.
The autism pharmaceutical market was worth $2.12 billion in 2020.
It was apparently worth $3.78 billion in 2021.
And in 2022 is was $6.94 billion.
Expected to be $7.41 billion in 2024.
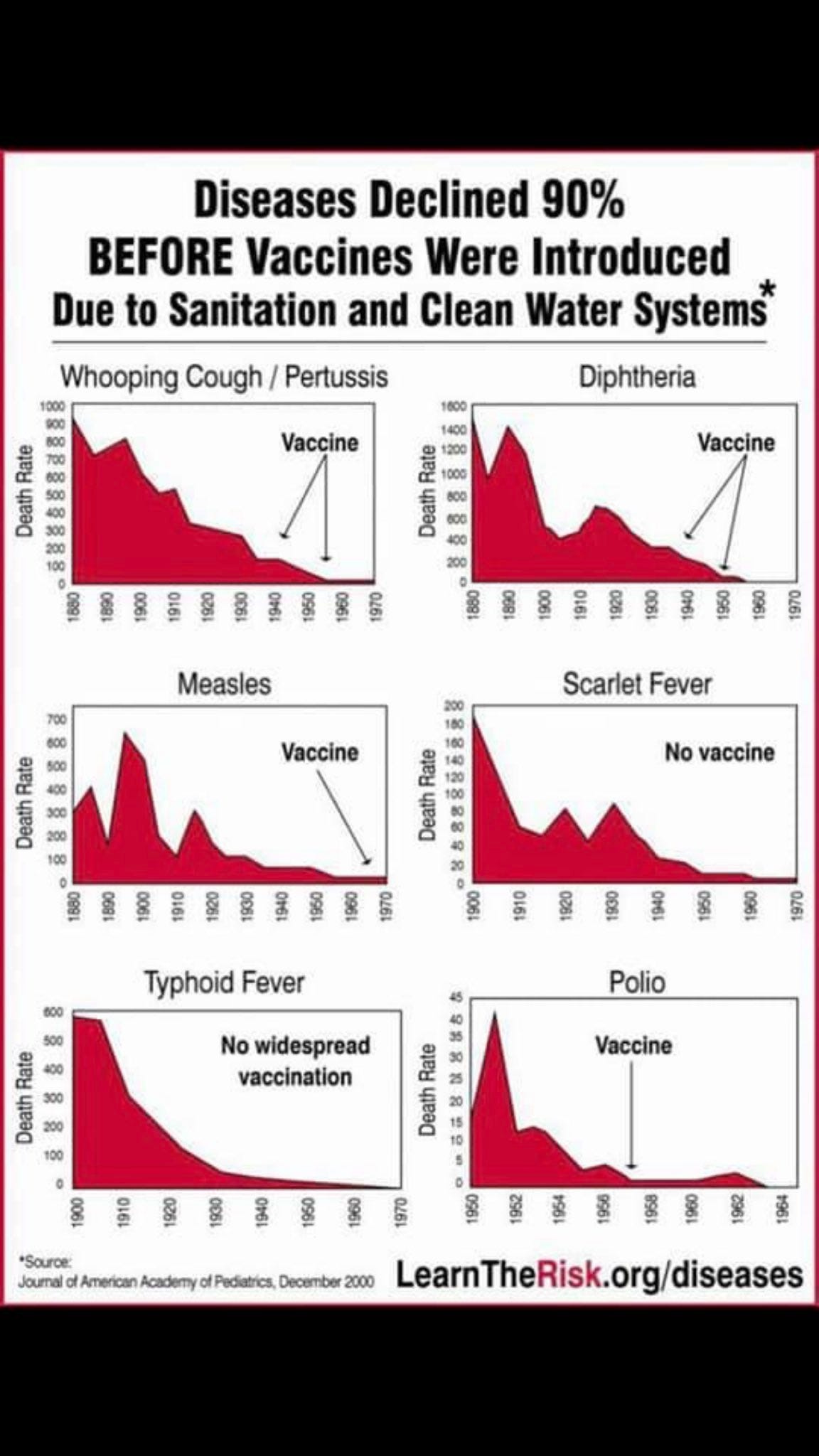
The MMR and all vaccines are unnecessary as these conditions were already in decline and deaths were virtually zero by the time the vaccines were introduced and there is no evidence that they are caused by viruses.
The symptoms of measles, mumps and rubella (and varicella) are the healing, not the disease, and should not be suppressed.
Our society will not be able to sustain the burden of ASD care for much longer. To say nothing of the sorrow and frustration felt by those who are suffer from ASD or who love someone who does. Pharma already makes a killing out of marketing the ever increasing number of vaccines. They also make a killing with drugs to treat the consequences.
The least we can do is talk about it.
🐒
References
1. Callous Disregard Andrew Wakefield
2.Dietary Considerations in Autism Spectrum Disorders: The Potential Role of Protein Digestion and Microbial Putrefaction in the Gut-Brain Axis
Megan R Sanctuary 1, Jennifer N Kain 2, Kathleen Angkustsiri 3 4, J Bruce German 5 6
Affiliations expand
PMID: 29868601
PMCID: PMC5968124
3.Sulforaphane treatment of autism spectrum disorder (ASD)
Kanwaljit Singh 1, Susan L Connors 2, Eric A Macklin 3, Kirby D Smith 4, Jed W Fahey 5, Paul Talalay 6, Andrew W Zimmerman 7
Affiliations expand
PMID: 25313065
PMCID: PMC4217462
Big Pharma gives with the one hand, and takes far more with the other. Clever business model they got there.
S-Methylmethionine in raw or very lightly cooked crucifers (brassica vegetables) would seem more likely helpful than nasty tasting sulforaphane. It restores deficient methylation. If the picky eaters won't eat the crucifers, one can buy synthetic SAM-e (S-adenosylmethionine).
BTW, metals can be toxicants, but not toxins. They aren't biologically secreted (with minor exception of bacterial methylation of mercury to the more toxic dimethylmercury). Please change 'neurotoxin' to 'neurotoxicant' unless in reference to an actual biologically produced poison.