
Vaccine efficacy

The Astra-Zeneca vaccine: gift or curse?
Far from being purely public spirited; saint Sarah Gilbert and her business partner Adrian Hill were set to make $20 million from the Astra Zeneca vaccine (if it hadn’t bombed) through their Vaccitech company’s first-to-market advantage. The AZ jab had an absolute efficacy of 1.2% at preventing common symptoms and a positive PCR result. It was tested against the meningitis jab, rather than inert placebo, which may also have affected the results. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. ‘There were 30 (0·5%) cases among 5807 participants in the vaccine arm and 101 (1·7%) cases among 5829 participants in the control group.’ Meaning that 98.3% of the control group didn’t get any symptoms during a major ‘pandemic’.

The Pfizer jab is bought in bucket loads by the UK government.
The Pfizer jab had an even worse efficacy of 0.7%. There were 8 cases out of 21720 (0.036%) with BNT 62b2 and 162 cases out of 21728 (0.74%) with placebo. 99.21% of people without the vaccine didn’t get symptoms plus positive PCR compared to 99.96% who got the jab. You decide if this small increase is worth the risk. Whistleblowers exposed how specimens were mislabelled and confused, casting very reasonable doubt on the validity of even this clinically insignificant and pathetic difference between treatment and control. Vaccine deaths during the trial were also later revealed to have been hidden in the appendix.
The 95% effectiveness measure was based on the claim that there were 162 ‘confirmed cases’ among the placebo participants compared to just 8 among the vaccinated participants. However, the study also reports that there were a much larger number of 'suspected but unconfirmed' cases and that these were more evenly spread between placebo participants (1,816 ie 8.3%) and vaccinated participants (1,594 ie 7.3%). This seems to suggest problems with blinding that led to a disproportionately small number of vaccinated with symptoms receiving PCR tests compared to placebo participants with symptoms, or as has been suggested by whistleblowers in the Pfizer PCR ‘testing’ labs, the samples were treated differently depending on whether they were test or control. If we discount the Drosten PCR entirely, as we should do because the sequences it was primed for have never been shown to associated with ‘covid’ let alone a validated test for it, this makes the relative efficacy of the jab ((1-test events/control events)x 100) just 12.5%- well below the cut off for the introduction of vaccines by the FDA and WHO, which is 50%.
The Moderna jab had an absolute efficacy of 1.14%; 15181 with mRNA-1273; 15170 with placebo; 11 cases in mRNA-1273 group; 185 cases in placebo, from the paper above.
The tiny effects of absolute efficacy were not reported in the MSM but rather the relative to placebo efficacy ie the 95% to 100% declared in the headlines. The efficacy demonstrated in trials run by pharma itself was in plain sight for anyone who read these papers at the beginning of December 2020. Though not many people seem to have done. A relative efficacy of 95% does not mean that only 5% get infected, nor that 100% of the control arm did.
Relative efficacy is 50% if, for example, 1% get symptoms on treatment arm compared to 2% on placebo arm. Relative vaccine efficacy = (1- no. cases in placebo group/no. of cases in treatment) x 100. Whatever the relative efficacy an absolute efficacy of 0.7% means that over 100 people had to be vaccinated to prevent 1 person from allegedly developing nonspecific symptoms or testing positive for nonspecific RNA sequences. The number needed to treat is the inverse of the absolute efficacy ie 100%/0.7%= 142. 142 people need to be jabbed with the Pfizer injectable to allegedly prevent one ‘case’ of ‘covid’.
Authors that challenge this dogma on vaccines are not, as a rule, published because the journals are entirely controlled by pharma. However, Peter Doshi, an editor of the BMJ, who can be described as an 'anti-vaxxer' as he opposes vaccine mandates, points out there is no evidence for the covid injectables due to Pfizer not releasing the raw data. He wrote 'Pfizer’s pivotal covid vaccine trial was funded by the company and designed, run, analysed, and authored by Pfizer employees. The company and the contract research organisations that carried out the trial hold all the data. And Pfizer has indicated that it will not begin entertaining requests for trial data until May 2025, 24 months after the primary study' 'Big pharma is the least trusted industry. At least three of the many companies making covid-19 vaccines have past criminal and civil settlements costing them billions of dollars. One pleaded guilty to fraud Other companies have no pre-covid track record. Now the covid pandemic has minted many new pharma billionaires, and vaccine manufacturers have reported tens of billions in revenue.' ‘Pharmaceutical companies are reaping vast profits without adequate independent scrutiny of their scientific claims. The purpose of regulators is not to dance to the tune of rich global corporations and enrich them further; it is to protect the health of their populations. We need complete data transparency for all studies, we need it in the public interest, and we need it now.'
Everyone knew that the jabs were not shown to prevent transmission of symptoms because transmission of symptoms by any natural route (other than injecting small mammals with toxic cell cultures directly into their noses, stomachs or brains and calling any pathology an infection) had never been demonstrated.
Finally, ‘Pfizer has been involved in several large settlements and fines, with one notable case resulting in a $2.3 billion settlement, the largest healthcare fraud settlement in the Department of Justice’s history at the time. This settlement included a $1.3 billion criminal fine and $1 billion in civil settlements. In another instance, Pfizer was fined £63.3 million by the Competition and Markets Authority (CMA) for overcharging the NHS for an epilepsy drug, with Flynn Pharma receiving an additional £6.7 million fine according to GOV.UK. Additionally, Pfizer’s subsidiary Biohaven paid nearly $60 million to resolve allegations of kickbacks to healthcare providers.’
Observational studies- what can they tell us?
Vaccine effectiveness is done on observational studies (some, but not all try to match vaccinated with unvaccinated for age, sex, care home etc) and is biased by many health factors of self-selection for vaccination, by the selection of the unvaccinated for the study, subsequent treatment, as well as the placebo effect (which accounts for up to 58% of the result). Calling observational studies 'real world' doesn't make them any more reliable.
This study of ‘real world data’ is from the National Institute of health and care Research in the Unit in Vaccines and Immunisation, who in collaboration with Imperial, who get shed loads from Bill and Mel to promote vaccines (and to write crazy mathematical lockdown models based on the ‘flu), and thus have a vested interest in showing effectiveness of vaccines to obtain more funding. They looked at an over 80s group of PCR positives. There were 13.13% deaths within 14 days of positive test in the unvaccinated group vs 12.35% in the Pfizer vaccinated group (though this number does not include those who died from the vaccine); an improvement of 0.95%. There were 15.35% of ‘cases’ unvaccinated admitted to hospital within 21 days of test and 14.43% vaccinated (though this does not include adverse events due to the vaccine); an improvement of 0.92% for Pfizer and 0.34% for AZ. When vaccine adverse events are added in, vaccines would show zero or negative efficacy.
Bias factors include the fact that those with ‘covid’ were prevented from being vaccinated, meaning that the unvaccinated group were already more sickly. It is also likely that the vaccinated weren’t given anti-virals or other such harmful inventions once they tested positive.
A difference in outcomes was noted depending on if the PCR ‘test’ positive came before or after the 14th day post-jab, with symptoms more likely to occur before 14 days were up, with worse outcomes, compared to after 14 days. If the mRNA is being translated into the spike protein and antibodies are being produced; symptoms of detox would be suppressed 14 days from the jab. This lack of symptoms and thus less hospitalisation, even though PCR ‘positive’, may mean less harmful treatments and less death. Not because disease is being avoided but because the spike protein is produced by the body under stress as part of the homeostatic mechanism. Dampening it down with antibodies is not a good idea at all. Neither is forced ventilation, anti-virals, isolation nor midazolam.
Vaccine effectiveness is the ratio of 'covid' PCR positive cases of respiratory symptoms vs PCR negative cases of respiratory symptoms comparing vaccinated with unvaccinated. The formula is VE=1- OR. OR= positives with vaccine/positives without vaccine divided by negatives with vaccine/negative without vaccine. If VE is below 1 the vaccinated had an increased chance of having their symptoms 'caused' by something other than 'SARS2’. In the above study of 156,000 people with self-reported symptoms of ‘covid’ 17,000 were unvaccinated and 138,000 were vaccinated. Having one group smaller than the other will skew the results. The VE was 0.84. But what is then causing the vaccinated’s 'covid' symptoms if they are mostly ‘covid’ PCR negative? The ‘‘flu’? And how is this an improvement in avoiding disease? It is, of course, possible that if the mRNA is being translated and antibodies are being produced that the body will be trying to detox using symptoms produced by other proteins that the ones chosen to prime the PCR, thus the vaccinated with symptoms will test negative more often.
Norman Fenton commented on the Israeli observational trial that eight of the authors hold stock or stock options with Pfizer and that the lead author was involved in the collaboration with Israel MOH to jointly approve anything that was published.
‘JMM, FJA, FK, GM, KP, JS, DLS, and LJ (ie 8 out of 15) hold stock and stock options in Pfizer. ML has provided advice on COVID-19 free of charge to Janssen, AstraZeneca, Pfizer, COVAXX (United Biomedical), and to the non-profit organisation One Day Sooner; has received consulting income or honoraria from Merck, Bristol Meyers Squibb, Sanofi, and Morris-Singer Fund; and had received institutional research support from Pfizer. All other authors declare no competing interests (though Alroy-Preis, the lead author, lied).’
‘Before discussing the flaws in the study, it is worth noting that, even if we accept as undisputed the number for 'Covid-19 related deaths' in the Israel study (715 among the unvaccinated and 138 among the vaccinated), then the absolute percentage increase in risk of death for an unvaccinated person is just 0.036%. That means that, even if we accept the 95% effectiveness measure, for every 10,000 unvaccinated people who catch Covid-19, about 3 or 4 would die as a result of not being vaccinated (or if the ‘infection’ fatality rate is 1 in 25 it would be 1 in 25.23 after vaccination). Critically, however, the paper does not provide any information about the number of adverse reactions - in particular the number of deaths - due to the vaccine. Hence, it does not provide the necessary information to make an informed decision about the overall risk/benefit of the vaccine.’
Fenton points out that declining ‘infection rates’ would make the calculation 74% not 95% effective as claimed. Cases before ‘full’ vaccination were ignored (decreasing the vaccinated cohort compared to the unvaccinated), thus increasing vaccine efficacy without the vaccine doing anything. He also shows that the vaccinated became exempt from being tested meaning that one in six vaccinated people received a PCR test and on average each unvaccinated person received two PCR tests. This alone would account for the 74% relative efficacy of the vaccine; without the vaccine doing anything. And as we have seen PCR positives led to isolation, hospitalisations, ventilation, anti-viral treatments and death, no wonder the much tested unvaccinated came off the worst.
What does wikipedia say about it?
Lastly a word about pharma marketing website Wikipedia who list number of lives saved by vaccines. It’s nonsense.

This is the important table from the paper that they are quoting for 20th century average annual deaths. NB Efficacy studies can’t be done on observational studies, only placebo controlled ones. Wikipedia are also using historical records and estimates. What was classified then as eg ‘smallpox’ may not be classified as such now.
You will see that they cherry pick short periods which show low or high deaths as required and not the decade as a whole. The years picked can be either after the introduction of the vaccine, around the same time or just before, they are not consistent and nor can they show that any change in deaths/cases were due to the vaccine and not the many other variables that affect health.
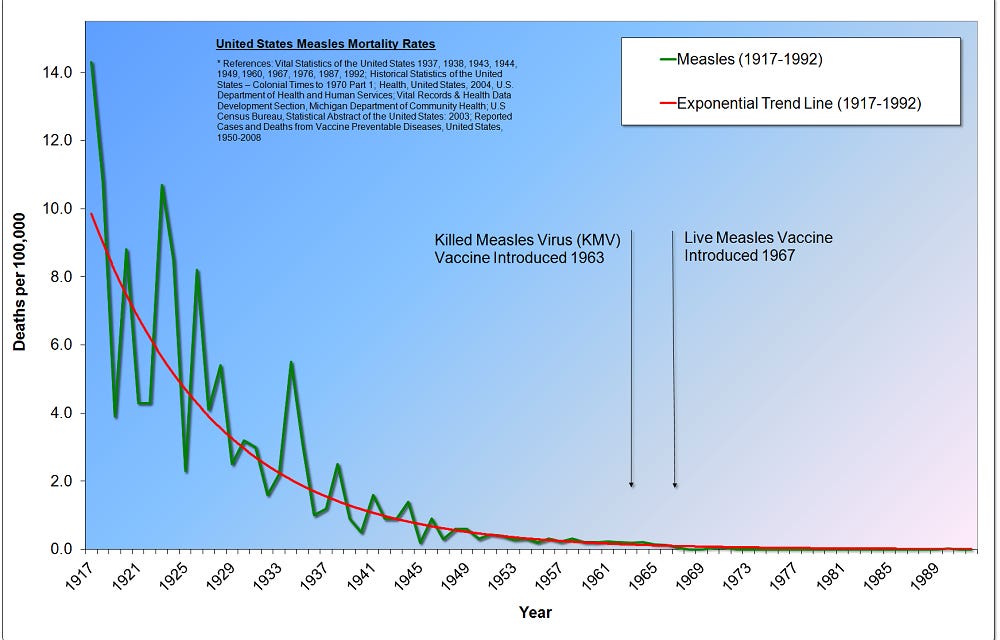
The table doesn't indicate, for example, that deaths for measles which was only 440 on average in the US between 1953 to 1962 was, in fact, itself a massive decline in deaths from the 19th century and early 20th and by 1968, when full introduction of the vaccine occurred, deaths were already even lower than those of 1953-62.
Most of the periods chosen only go up to the 1950s and since then standards of living, housing and hygiene have improved considerably and DDT etc etc has been banned.
The CDC and whooping cough- criminal disingenuity?
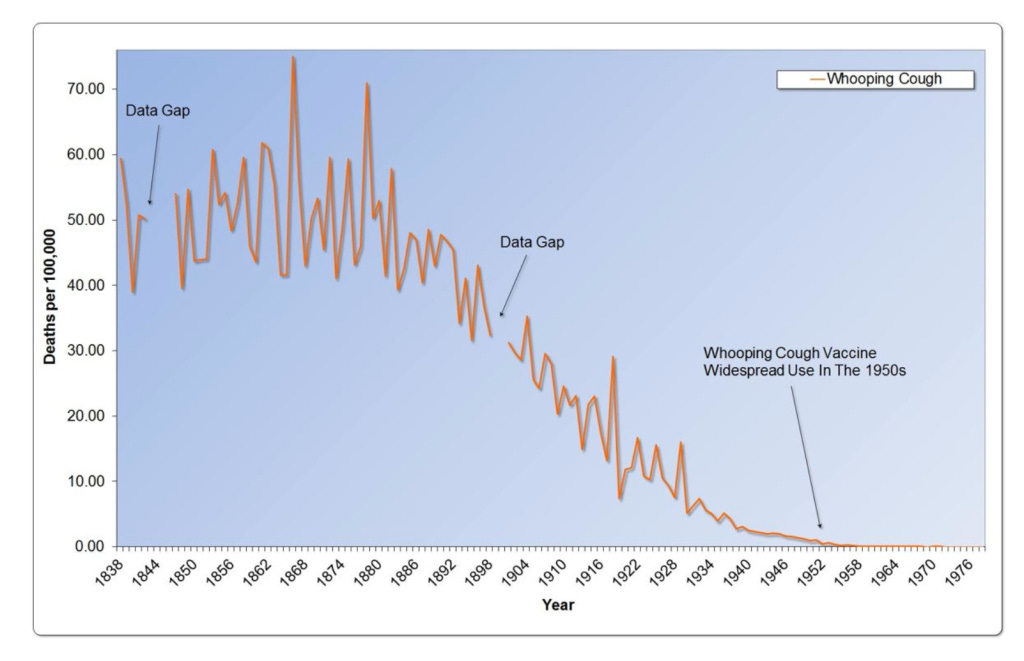
Whooping cough, or pertussis, is a toxin-mediated bacterial disease. Here are the whooping cough deaths for England and Wales 1838 to 1978. As you can see deaths were already nearly zero by the time the vaccine was introduced.
Here are the CDC’s numbers for the United States 1922 to 2022. As you can see cases increased slightly in the 2010s despite vaccines rates remaining high. It was put down to waning immunity from the vaccine. However, the highest incidence in the 2012 peak was in vaccinated children and there was no significant difference in attack rates between vaccinated, under vaccinated or unvaccinated children. However, the CDC called of vaccination of pregnant women to pass on ‘immunity’ to newborns- although newborns would only have short lived protection via placenta or breast milk. Breast feeding itself, without vaccination, and with vitamin C, has been shown to protect babies from prolonged coughing symptoms, and is risk free.
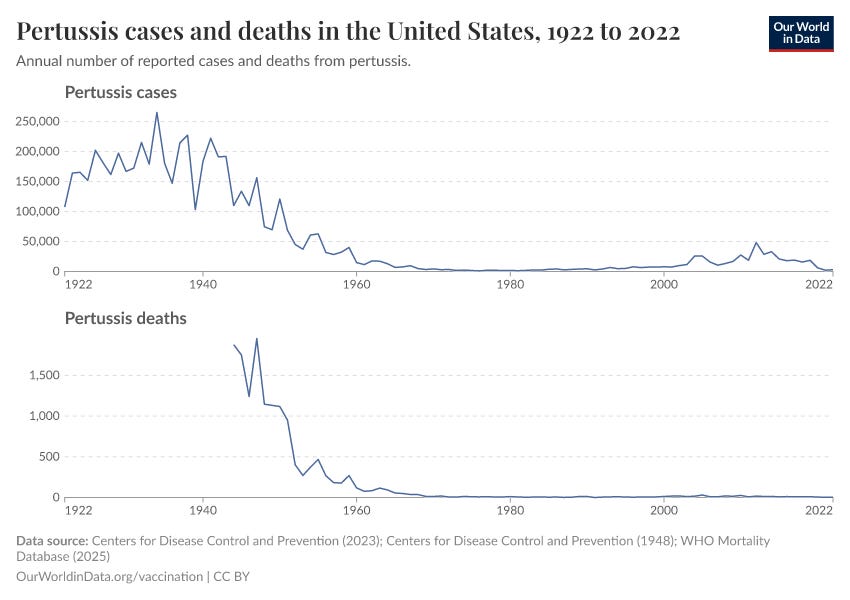
Look at the graph above again and see the deaths from whooping cough provided by the CDC. Note that the axis starts at 1922 but the data is missing. Why do you think that is?
This is whooping cough mortality from 1900 to 1957 in the United States.
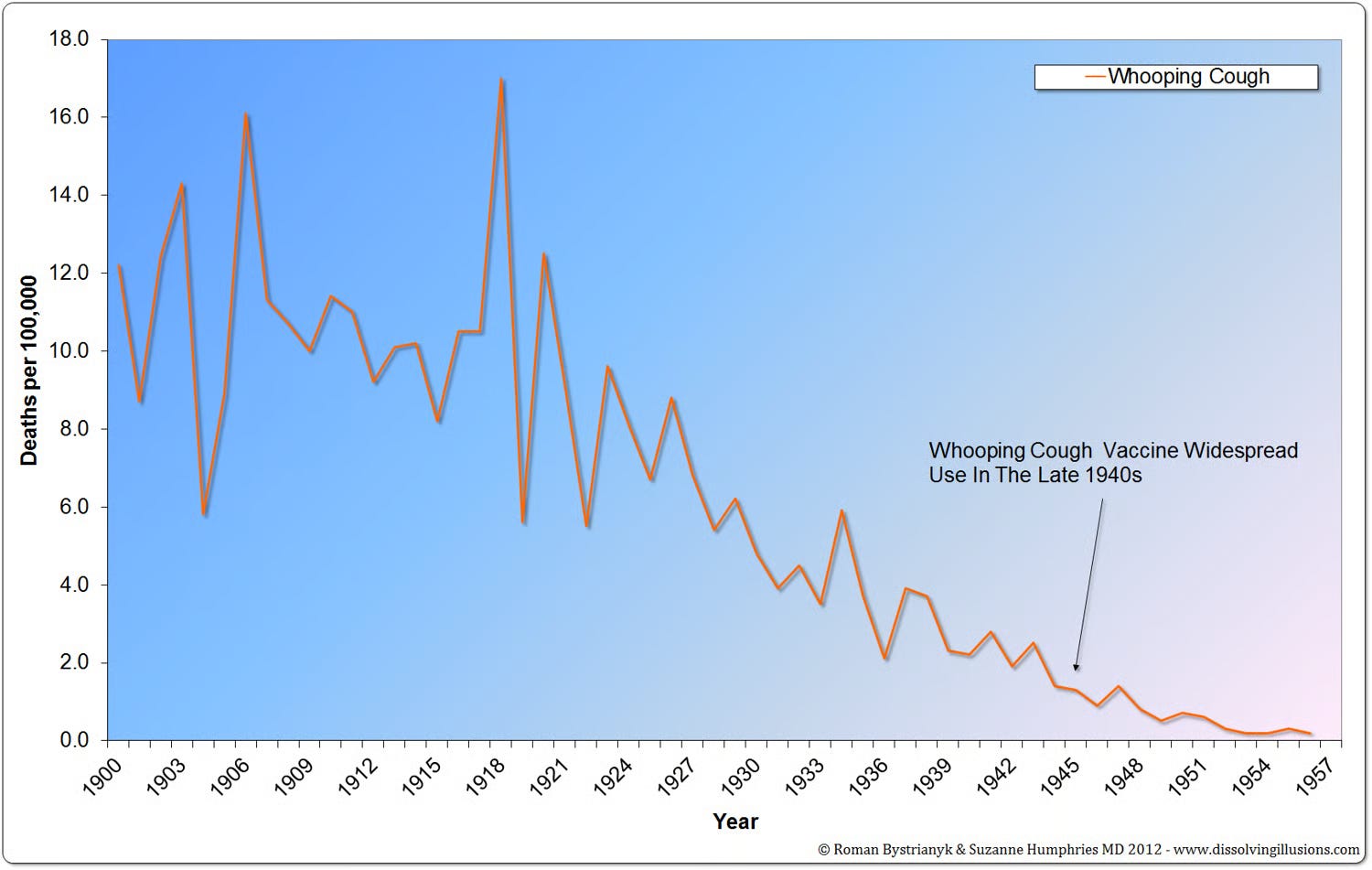
Find the years before 1942 (before which the CDC data is missing). What do you see?
There is, and never was, any evidence for vaccination.
🐒
Too bloody right
So, basically, it suppressed the detox process of a few folk, and killed a few folk more. Winning!(?)